Bladder cancer
Bladder cancer is an uncontrolled, abnormal growth and multiplication of cancerous cells that typically manifest on the urothelium. The most prevalent presenting symptom of bladder cancer is painless macroscopic haematuria (visible blood in the urine).
Expand all
Collapse all
Definition
Bladder cancer is an uncontrolled, abnormal growth and multiplication of cancerous cells that typically manifest on the urothelium, the inner lining of the bladder wall (Cancer Research UK, 2023).
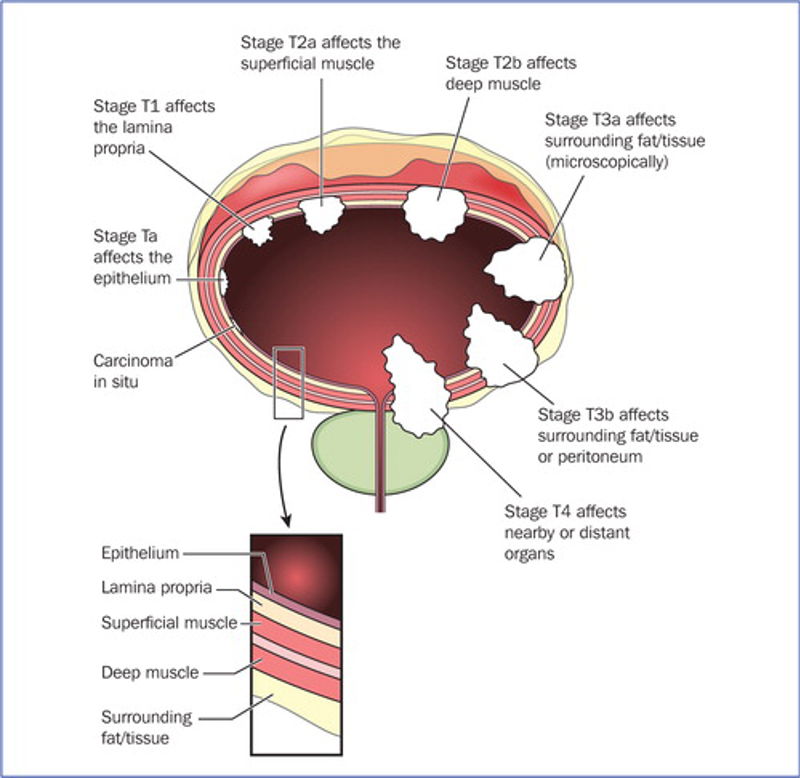
The urinary tract consists of the kidneys, ureters, bladder and urethra. The bladder is a hollow, muscular organ situated at the base of the pelvis in the urinary tract. Its layers consist of:
- urothelium (a form of transitional epithelium)
- peritoneum
- lamina propria
- mucosa
- superficial muscle
- deep muscle
- peri-vesical tissue (fatty layer) (Brooker and Nicol, 2011) (Figure 1)
Bladder cancer is the most prevalent malignancy of the urinary tract (Cancer Research UK, 2023). It is the 10th most common cancer in the
To view the rest of this content please log in
Symptoms
The most prevalent presenting symptom of bladder cancer is painless macroscopic haematuria (visible blood in the urine), which affects 80% of male patients and 70% of female patients, and microscopic haematuria (non-visible blood, dipstick positive) (Babjuk et al, 2018). Around 15% of patients will exhibit symptoms linked to the lower urinary tract, including:
- urgency
- dysuria
- increased frequency
- pelvic discomfort in cases of more advanced tumours and urinary tract obstruction (Witjes et al, 2023)
To view the rest of this content please log in
Aetiology
There are various forms of bladder cancer, but the most frequent type, accounting for 95% of bladder neoplasms, is urothelial carcinoma, also known as transitional cell carcinoma (National Institute for Health and Care Excellence, 2015). Rarer forms of bladder cancer include:
- sarcoma
- small cell bladder cancer
- adenocarcinoma (Cancer Commons, 2020; Cancer Research UK, 2023)
Bladder cancer development is linked to several risk factors. Smoking is the most well-established risk factor, increasing the risk of bladder cancer by up to four times that of a person who has never smoked (Cancer Research UK, 2023). Other risk factors include:
- radiation
- exposure to specific industrial chemicals
- ageing
- family history (Babjuk et al, 2018; Witjes et al, 2023)
Raising awareness of the advantages of quitting smoking is vital to reducing the risk of tumour recurrence and advancement as well as to improve general health (Anderson, 2018a, b; Witjes et al, 2023).
To view the rest of this content please log in
Diagnosis
Diagnosing bladder cancer typically begins with an urgent GP referral, as per the most recent NHS England (2023) guidelines. This comprises a comprehensive assessment, subsequent diagnostics and/or investigations, grading and staging to confirm the extent of the disease (Table 1), and initiating care appropriately and promptly (Babjuk et al, 2018).
| Table 1. Assessment, diagnostics and investigations for bladder cancer | |
| Assessment | Diagnostics and staging |
| Non-muscle invasive bladder cancer | |
|
Patient history: urinary tract symptoms, trauma, renal disease, medication
Physical assessment: abdominal, vaginal, blood pressure
Blood tests: urea/electrolytes, creatinine |
Cystoscopy, transurethral resection of bladder tumour, urine cytology, retrograde pyelogram, bladder biopsy
|
|
Initial work-up in patients with haematuria |
Renal and bladder ultrasound scan
|
|
Initial diagnosis of non-muscle invasive bladder cancer
|
Computed tomography urography should be performed only in selected cases (eg tumours located in the trigone, multiple- or high-risk tumours)
|
|
In all patients with symptoms | |
To view the rest of this content please log in
Treatment
The management and treatment of non-muscle-invasive bladder cancer, muscle-invasive bladder cancer, locally advanced and advanced/metastatic diseases depend on several factors, including:
- patient's age
- disease grade and stage
- suitability and appropriateness of the chosen treatment (Witjes et al, 2023)
Treatment options include transurethral resection of the bladder tumour, which is typically the first-line treatment and can be curative for non-muscle-invasive disease (Babjuk et al, 2018), and cystoscopy, which is considered the ‘gold standard’ in the initial diagnosis of bladder cancer (Cancer Research UK, 2023).
Additional treatments consist of cystectomy, systemic chemotherapy, radiation and chemo-radiation therapy, biological therapy and intravesical medicines (drugs administered directly into the bladder using a urethral catheter) (Vahr et al, 2015). Although there are numerous types of immunotherapies and chemotherapy, the two most common treatments for non-muscle-invasive bladder cancer are bacillus-calmette guerin (immunotherapy) and mitomycin-C (chemotherapy) (Babjuk et al, 2018). Bacillus-calmette guerin is the conventional treatment for carcinoma
To view the rest of this content please log in
NMC proficiencies
Nursing and Midwifery Council: standards of proficiency for registered nurses
Part 1: Procedures for assessing people’s needs for person-centred care
1. Use evidence-based, best practice approaches to take a history, observe, recognise, and accurately assess people of all ages
1.1.1 signs of mental and emotional distress or vulnerability
Part 2: Procedures for the planning, provision, and management of person-centred nursing care
11.1. carry out initial and continued assessments of people receiving care and their ability to self-administer their own medications.
To view the rest of this content please log in
Resources
Anderson B. Bladder cancer: overview and disease management. Part 1: non-muscle-invasive bladder cancer. Br J Nurs. 2018a;27(9):S27-S37. https://doi.org/10.12968/bjon.2018.27.9.S27
Anderson B. Bladder cancer: overview and management. Part 2: muscle-invasive and metastatic bladder cancer. 2018b;27(18):S8-S20. https://doi.org/10.12968/bjon.2018.27.18.S8
Babjuk M, Burger M, Compérat E et al. EAU guidelines on non-muscle-invasive bladder cancer (TAT1 and CIS). 2018. https://d56bochluxqnz.cloudfront.net/documents/EAU-Guidelines-Non-muscle-invasive-Bladder-Cancer-2018.pdf (accessed 19 April 2024)
Brooker C, Nicol M. Alexander's nursing practice. 4th edn. Edinburgh: Churchill Livingstone/Elsevier; 2011
Cancer Commons. New treatments for bladder cancer in 2020. 2020. https://cancercommons.org/latest-insights/new-treatments-for-bladder-cancer-in-2020/ (accessed 19 April 2024)
Cancer Research UK. Risks and causes of bladder cancer. 2023. http://www.cancerresearchuk.org/about-cancer/bladder-cancer/risks-causes (accessed 19 April 2024)
Di Stasi SM, Valenti M, Verri C et al. Electromotive instillation of mitomycin immediately before transurethral resection for patients with primary urothelial non-muscle invasive bladder cancer: a randomised controlled trial. Lancet Oncol. 2011;12(9):871-879. https://doi.org/10.1016/S1470-2045(11)70190-5
Lammers RJ, Witjes JA, Inman BA et al. The role of a combined regimen with intravesical chemotherapy and hyperthermia in the management of non-muscle-invasive bladder cancer: a systematic review. Eur Urol. 2011;60(1):81-93.
To view the rest of this content please log in