Expand all
Collapse all
Purpose
The term 'airway’ describes the anatomical structures that join the nose and mouth to the lungs (Marieb and Keller, 2021). A patent airway is essential to life; if air cannot reach the lungs, death occurs within minutes (Resuscitation Council UK, 2021). Problems with the airway are common in acute areas of care, and especially so when patients are critically ill.
Airway obstruction can be partial or complete (McPherson and Stephens, 2012). In partial obstruction, the flow of air to the lungs is reduced and abnormal sounds such as snoring, gurgling or wheezing may be produced (Resuscitation Council UK, 2021). The patient may become hypoxic if there is inadequate air flow to the lungs.
In complete airway obstruction, no air reaches the alveoli. The chest is silent, breath sounds at the mouth are absent, and profound hypoxia occurs rapidly. Without intervention, the person will die within a few minutes (Resuscitation Council
To view the rest of this content please log in
Assessment
Causes of airway obstruction
The common causes of airway obstruction include:
- reduced level of consciousness (obstruction by soft palate, epiglottis, tongue)
- vomit
- blood
- excessive secretions
- regurgitation of stomach contents
- airway trauma
- foreign body
- oedema as a result of burns, inflammation or anaphylaxis
- laryngospasm
- bronchospasm
- pulmonary oedema
- external compression of the airway (tumour, haematoma, trauma)
- blocked tracheostomy tube
Of these, reduced consciousness level, fluid or other matter in the airway, and inflammation are the most commonly encountered (McPherson and Stephens, 2012).
Assessment of the airway
A person who can talk in sentences, with no abnormal airway sounds, is likely to have a patent airway (Cathala and Moorley, 2020). Speaking to the patient, and eliciting a response, is therefore a good initial assessment in the conscious patient. For individuals who are not fully conscious, or when there is doubt about the patency of the airway, a look-listen-feel approach is recommended:
- Look for
To view the rest of this content please log in
Procedure
Opening the airway
Opening the airway means positioning the head and neck so that the airway is as straight as possible, and lifting the jaw to move the tongue away from the back of the pharynx (McPherson and Stephens, 2012). Before this is attempted, any visible obstruction should be removed.
Start by opening the mouth and looking inside. If there are fluids or semi-solid matter in the mouth or pharynx, try to remove them using suction (Resuscitation Council UK, 2021). Note that suctioning the airway is an aerosol-generating procedure, so precautions must be taken to reduce the risk of airborne transmission of potentially infectious material. Other airway procedures that are aerosol-generating include tracheal intubation and extubation, manual ventilation, non-invasive ventilation, and high-flow nasal oxygen.
If an obstruction in the mouth or pharynx is too solid to remove with suction, Magill's forceps may be useful. These are usually found on the
To view the rest of this content please log in
Equipment
The following equipment is used for airway management, depending on the patient and circumstances:
- oropharyngeal airways (Figure 4)
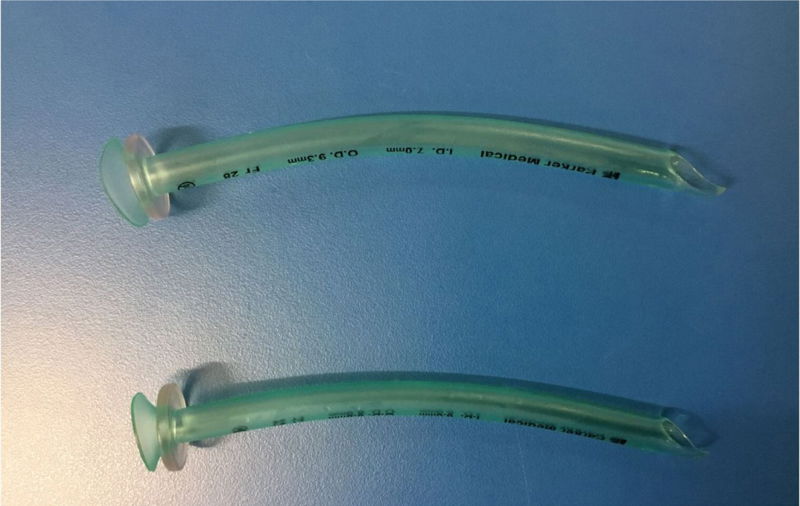
- nasopharyngeal airway (Figure 5)
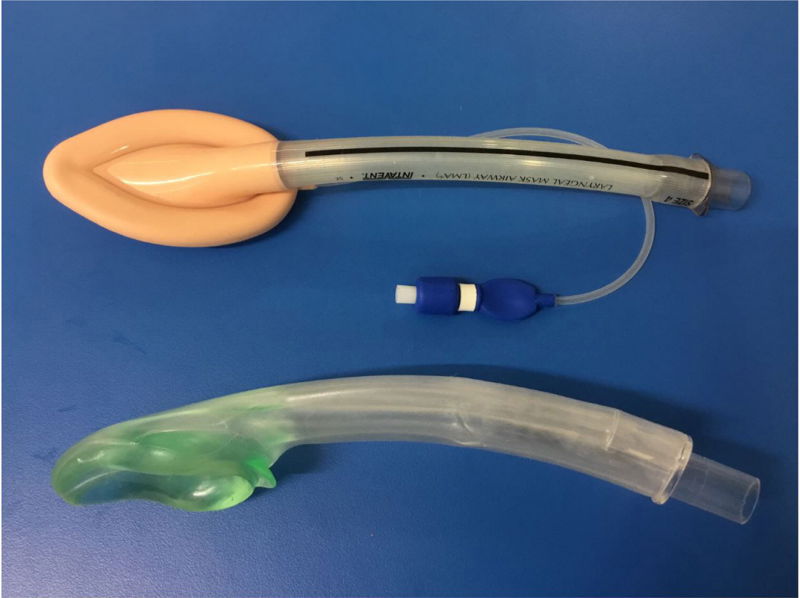
- supraglottic airway devices (Figure 6)
- endotracheal tubes (Figure 7)
Refer to local guidance when choosing which equipment to use in airway management.

To view the rest of this content please log in
Next steps
People who are critically ill often have multiple risk factors for airway compromise, making airway management a core skill for clinicians involved in their care. Recognising the patient at risk of airway compromise, and performing an accurate assessment using a look-listen-feel approach are key aspects of airway management. These skills must be supported by a knowledge of simple methods to clear the airway, and of devices that may be used to maintain airway patency. While this article has given an overview of the topic, further reading and practical training in airway management are recommended. Clinicians should also ensure they are up to date with current recommendations for infection control, as a number of airway interventions are aerosol generating.
To view the rest of this content please log in
NMC proficiencies
Nursing and Midwifery Council: standards of proficiency for registered nurses
Part 1: Procedures for assessing people’s needs for person-centred care
2.16 recognise and manage seizures, choking and anaphylaxis, providing appropriate basic life support
Part 2: Procedures for the planning, provision and management of person-centred nursing care
8. Use evidence-based, best practice approaches for meeting needs for respiratory care and support, accurately assessing the person’s capacity for independence and self-care and initiating appropriate interventions
8.6 manage airway and respiratory processes and equipment
To view the rest of this content please log in
Resources
Marieb E, Keller S. Essentials of human anatomy & physiology. 13th edn. London: Pearson; 2021
Resuscitation Council UK. Advanced life support. 8th edn. London, Resuscitation Council UK; 2021
To view the rest of this content please log in